
Breast reconstruction with flap surgery
Overview
Breast reconstruction is a surgical procedure that restores shape to your breast after a mastectomy — surgery that removes your breast to treat or prevent breast cancer. Breast reconstruction with flap surgery involves taking a section of tissue from one area of your body — most often your abdomen — and relocating it to create a new breast mound.
Breast reconstruction with flap surgery is a complex procedure performed by a plastic surgeon. Much of the breast reconstruction using your body's own tissue can be accomplished at the time of your mastectomy (immediate reconstruction), though sometimes it can be done as a separate procedure later (delayed reconstruction).
Your plastic surgeon may recommend a two-stage procedure. The first stage is to place an implant expander and the second stage is to complete the tissue reconstruction.You'll likely need another operation to perform nipple reconstruction.
Risks
Breast reconstruction with flap surgery is a major procedure and carries with it the possibility of significant complications, including:
- Changes in breast sensation
- Prolonged time in surgery and under anesthesia
- Extended recovery and healing time
- Poor wound healing
- Fluid collection (seroma)
- Infection
- Bleeding
- Tissue death (necrosis) due to insufficient blood supply
- Loss of sensation at the tissue donor site
- Abdominal wall hernia or weakness
Radiation therapy delivered to the skin and chest wall may pose complications during healing if it's given after breast reconstruction surgery. Your doctor may recommend waiting until you're finished with radiation therapy before proceeding with the second stage of the breast reconstruction.
How you prepare
Before a mastectomy, your doctor may recommend that you meet with a plastic surgeon. Consult a plastic surgeon who's board certified and experienced in breast reconstruction following mastectomy. Ideally, your breast surgeon and the plastic surgeon should work together to develop the best surgical treatment and breast reconstruction strategy in your situation.
Your plastic surgeon will describe your surgical options and may show you photos of women who have had different types of breast reconstruction. Your body type, health status and cancer treatment factor into which type of reconstruction will give you the best result. The plastic surgeon also provides information on anesthesia, where the operation will be performed and what kind of follow-up procedures may be necessary.
Your plastic surgeon may discuss the pros and cons of surgery on your opposite breast, even if it's healthy, so that it more closely matches the shape and size of your reconstructed breast. Surgery to remove your healthy breast (contralateral prophylactic mastectomy) can double the risk of surgical complications, such as bleeding and infection. Also, there may be less satisfaction with cosmetic outcomes after surgery.
Before surgery, follow your doctor's instructions on preparing for the procedure. This may include guidelines on eating and drinking, adjusting current medications, and quitting smoking.
What you can expect
Chances are your new breast won't look exactly like your natural one did. However, the contour of your new breast can usually be restored so that your silhouette looks similar to your silhouette before surgery.
Breast reconstruction with flap surgery is the most complex breast reconstructive option. Your surgeon transfers a section of skin, muscle, fat and blood vessels from one part of your body to your chest to create a new breast mound. In some cases, the skin and tissue need to be augmented with a breast implant to achieve the desired breast size.
Surgical methods
Autologous tissue breast reconstruction uses one of two surgical methods:
- Pedicled flap surgery The surgeon cuts some of the blood vessels to the tissue to be transferred but keeps other blood vessels intact. Tunneling the tissue beneath your skin to your chest area, the surgeon then creates the new breast mound or pocket for the implant.
- Free flap surgery. The surgeon disconnects the tissue completely from its blood supply and reattaches the tissue to new blood vessels near your chest. Because of reattaching blood vessels, free flap surgery typically takes longer than does pedicled flap surgery.
Types of flap surgery
The tissue for reconstructing your breast most often comes from your abdomen. Tissue from your back or — less commonly — your buttocks may also be used. Your surgeon determines which method is best for you based on your body type and your medical and surgical history.
-
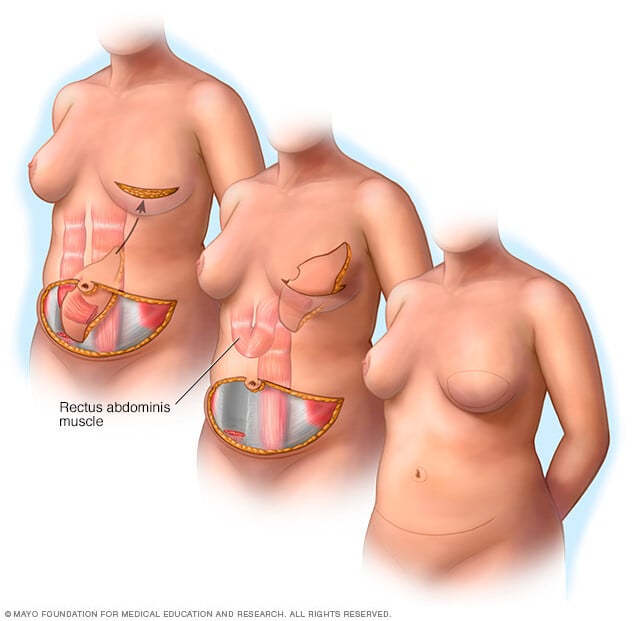
Abdomen (TRAM flap). Your surgeon removes tissue — including muscle — from your abdomen in a procedure known as a transverse rectus abdominis muscle (TRAM) flap. The TRAM flap can be transferred as a free flap or a pedicled flap.
A pedicled TRAM flap uses your whole rectus muscle — one of the four major muscles in your abdomen. For a muscle-sparing free TRAM flap, your surgeon takes only a portion of your rectus abdominis muscle, which may help you retain abdominal strength after surgery.
-
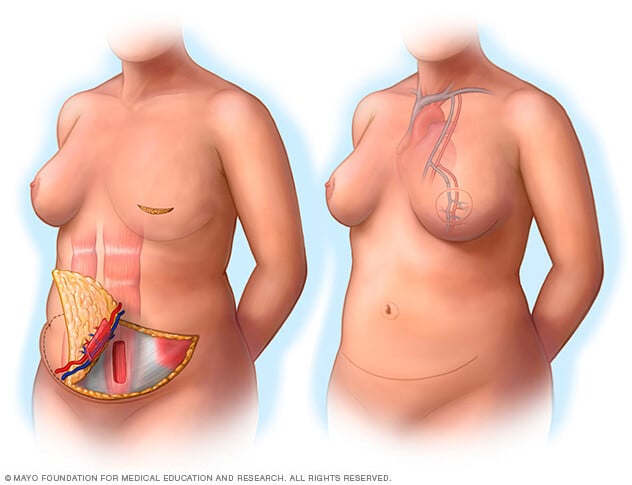
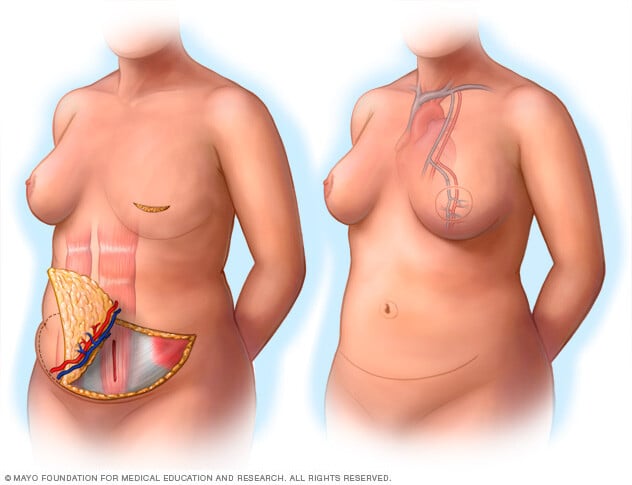
Abdomen (DIEP flap). A newer procedure, deep inferior epigastric perforator (DIEP) flap, is similar to an msTRAM flap, but only skin and fat are removed. Most of the abdominal muscle is left in place and minimal muscle tissue is taken to form the new breast mound. Reattaching blood vessels requires expertise in surgery through a microscope (microsurgery).
An advantage to this type of breast reconstruction is that you'll retain more strength in your abdomen. If your surgeon can't perform a DIEP flap procedure for anatomical reasons, he or she might opt for the msTRAM procedure instead.
- Abdomen (SIEA flap). A variation of the DIEP flap, the superficial inferior epigastric artery (SIEA) flap uses the same abdominal tissue but relies on blood vessels that aren't as deep within the abdomen. This provides a less invasive option, but not all women's SIEA blood vessels are adequate for this type of flap surgery.
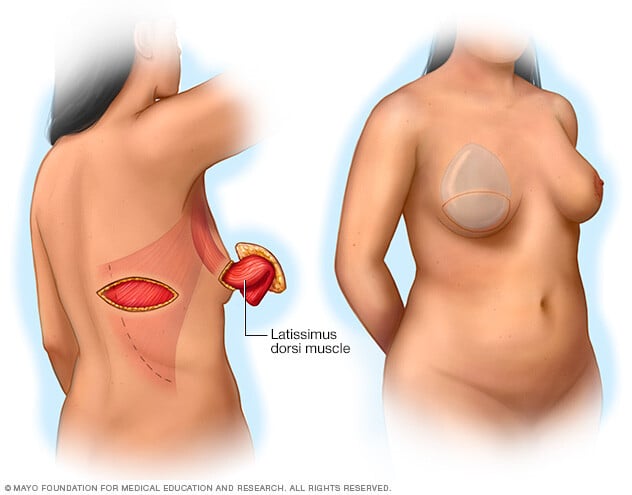
- Back (latissimus dorsi flap). This surgical technique takes skin, fat and muscle from your upper back, tunneling it under your skin to your chest. Because the amount of skin and other tissue is generally less than in a TRAM flap surgery, this approach may be used for small and medium-sized breasts or for creating a pocket for a breast implant. Although uncommon, some women experience muscle weakness in the back, shoulder or arm after this surgery.
- Buttocks (gluteal flap). A gluteal flap is a free flap procedure that takes tissue from your buttocks and transplants it to your chest area. A gluteal flap may be an option for women who prefer tissue reconstruction but who don't have enough extra tissue in their backs or abdomens.
- Inner thigh (TUG). Another newer option, the transverse upper gracilis (TUG) flap, uses muscle and fatty tissue from the bottom of the buttocks to the inner thigh. TUG flap surgery, which isn't available everywhere, may be an option for women whose thighs touch and who have small to medium-sized breasts.
Because adequate blood supply is critical to the survival of transplanted tissue in flap surgery, your surgeon may prefer not to perform a pedicled flap procedure if you're a smoker or if you have diabetes, vascular disease or a connective tissue disorder. If you smoke, you may be asked to quit for four to six weeks before your surgery. Also, obesity may preclude you from having a pedicled TRAM flap.
In general, flap breast reconstruction surgery is more extensive than is mastectomy or implant reconstruction. Flap procedures result in larger incisions that take longer to heal, so they require a longer recovery period and may require a longer hospital stay.
A new technique for breast reconstruction, autologous fat grafting, uses liposuction to gather fat tissue from your thighs, abdomen or buttocks to reconstruct the breast or to improve the appearance of your breast after reconstruction.
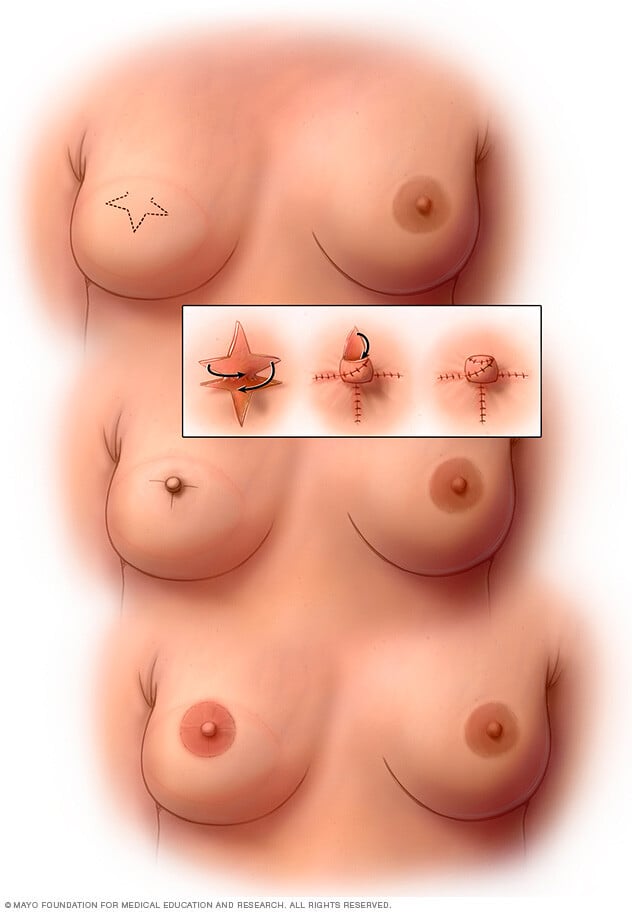
Nipple reconstruction
Breast reconstruction may also entail reconstruction of your nipple, if you choose, including tattooing to define the dark area of skin surrounding your nipple (areola).
Recovery
You may be tired and sore for a few weeks after your surgery. Your doctor can prescribe medication to control your pain. You may have drainage tubes in place for a short time after your surgery to remove excess fluids that collect in the surgical site.
Wearing an elastic bandage or support bra can help keep swelling down and support your breast while it heals.
You'll also have stitches (sutures) after your surgery. They'll probably be absorbable sutures, though, so you won't need to have them removed. Scarring is permanent, but the scars generally fade over time.
Getting back to normal activities may take up to six weeks or more. Your doctor will let you know of any restrictions to your activities, such as avoiding overhead lifting or strenuous physical activities. Don't be surprised if it seems to take a long time to bounce back from surgery — some women report that it takes as long as a year or two before feeling completely healed and back to normal.
Future breast cancer screening
If you've had only one breast reconstructed, you'll need to have screening mammography done regularly on your other breast. Mammography isn't necessary on breasts that have been reconstructed.
You may also choose to perform breast self-exams on your natural breast and the skin and surrounding area of your reconstructed breast. This may help you become familiar with the changes to your breast after surgery so that you can be alert to any new changes and report those to your doctor.
Results
Keep your expectations realistic about your surgery. Breast reconstruction offers many benefits, but it won't make your breast look or feel exactly like it did before your mastectomy.
What breast reconstruction can do:
- Give you a breast contour
- Help your breasts look natural under clothing or a bathing suit
- Help you avoid the need for using a form (external prosthesis) inside your bra
What breast reconstruction might do:
- Improve your self-esteem and body image
- Partially erase the physical reminders of your disease
- Require additional surgery to correct reconstructive problems
What breast reconstruction won't do:
- Make you look exactly the same as before
- Give your reconstructed breast the same sensations as your normal breast

