
Pulmonary edema
Overview
Pulmonary edema is a condition caused by too much fluid in the lungs. This fluid collects in the many air sacs in the lungs, making it difficult to breathe.
In most cases, heart problems cause pulmonary edema. But fluid can collect in the lungs for other reasons. These include pneumonia, contact with certain toxins, medications, trauma to the chest wall, and traveling to or exercising at high elevations.
Pulmonary edema that develops suddenly (acute pulmonary edema) is a medical emergency that needs immediate care. Pulmonary edema can sometimes cause death. Prompt treatment might help. Treatment for pulmonary edema depends on the cause but generally includes additional oxygen and medications.
Symptoms
Pulmonary edema symptoms may appear suddenly or develop over time. Symptoms depend on the type of pulmonary edema.
Sudden (acute) pulmonary edema symptoms
- Difficulty breathing (dyspnea) or extreme shortness of breath that worsens with activity or when lying down
- A feeling of suffocating or drowning that worsens when lying down
- A cough that produces frothy sputum that may have blood in it
- A rapid, irregular heartbeat (palpitations)
- Anxiety, restlessness or a feeling that something bad is about to happen
- Cold, clammy skin
- Wheezing or gasping for breath
Long-term (chronic) pulmonary edema signs and symptoms
- Awakening at night with a cough or breathless feeling that may be relieved by sitting up
- Difficulty breathing with activity or when lying flat
- Fatigue
- More shortness of breath than usual when you're physically active
- New or worsening cough
- Rapid weight gain
- Swelling in the legs and feet
- Wheezing
High-altitude pulmonary edema (HAPE) signs and symptoms
HAPE can occur in adults and children who travel to or exercise at high altitudes. Symptoms are similar to those that occur with acute pulmonary edema and can include:
- Headache, which may be the first symptom
- Shortness of breath with activity, which becomes shortness of breath at rest
- Not being able to exercise as much as you once could
- Dry cough, at first
- Later, a cough that produces frothy sputum that may look pink or have blood in it
- A very fast heartbeat (tachycardia)
- Weakness
- Chest pain
- Low fever
Symptoms of high-altitude pulmonary edema (HAPE) tend to get worse at night.
When to see a doctor
Pulmonary edema that comes on suddenly (acute pulmonary edema) is life-threatening. Call 911 or emergency medical help if you have any of the following acute symptoms:
- Shortness of breath, especially if it comes on suddenly
- Trouble breathing or a feeling of suffocating (dyspnea)
- A bubbly, wheezing or gasping sound when breathing
- Coughing up phlegm that looks pink or has blood in it
- Breathing difficulty with a lot of sweating
- A blue or gray color to the skin
- Confusion
- A big drop in blood pressure that causes lightheadedness, dizziness, weakness or sweating
- A sudden worsening of any of pulmonary edema symptoms
Don't drive yourself to the hospital. Instead, call 911 or emergency medical care and wait for help.
Causes
The causes of pulmonary edema vary. Pulmonary edema falls into two categories, depending on where the problem starts.
- If a heart problem causes the pulmonary edema, it's called cardiogenic pulmonary edema. Most often, the fluid buildup in the lungs is due to a heart condition.
- If pulmonary edema is not heart related, it's called noncardiogenic pulmonary edema.
- Sometimes, pulmonary edema can be caused by both a heart problem and a nonheart problem.
Understanding the relationship between the lungs and the heart can help explain why pulmonary edema may occur.
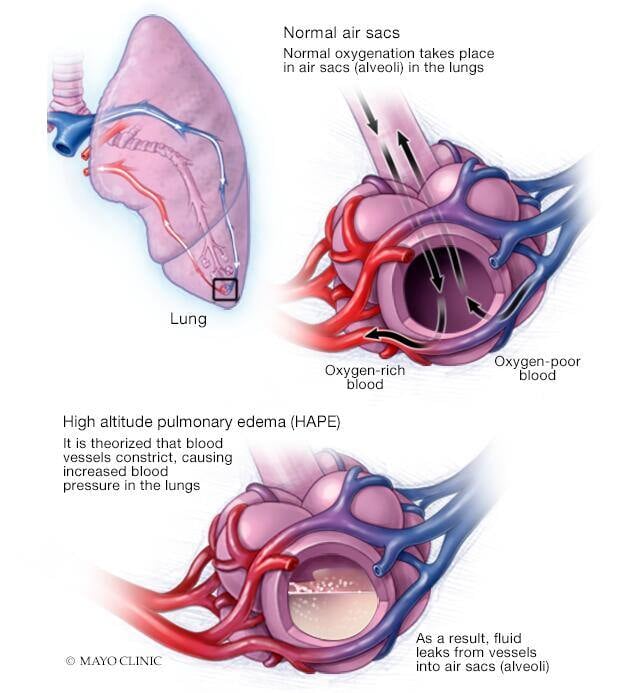
How the lungs work
Lungs contain many small, elastic air sacs called alveoli. With each breath, these air sacs take in oxygen and release carbon dioxide. Typically, this exchange of gases occurs without problems.
But sometimes, the alveoli fill with fluid instead of air. This keeps the bloodstream from taking in oxygen.
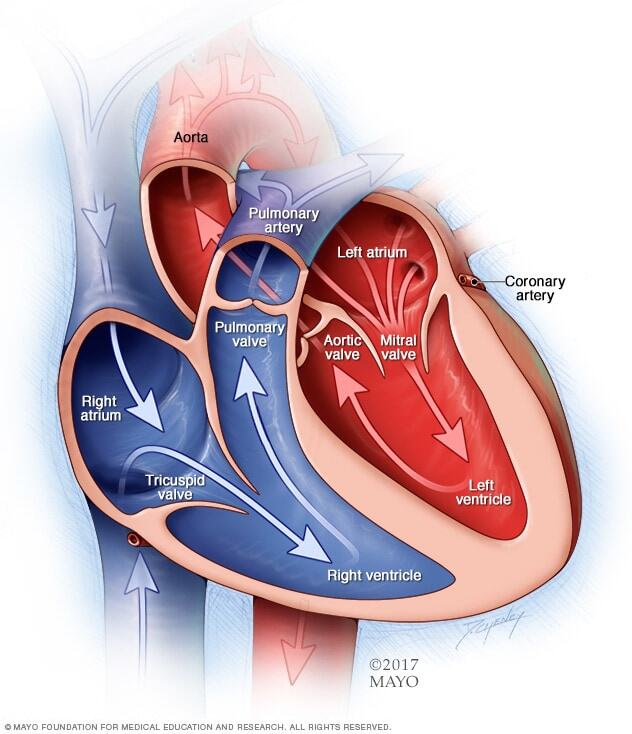
How the heart works
The typical heart is made of two upper and two lower chambers. The upper chambers (the right and left atria) receive incoming blood and pump it into the lower chambers (right and left ventricles). The lower chambers pump blood out of the heart.
Typically, blood without oxygen from all over the body enters the right atrium then the right ventricle. From there it's pumped through large blood vessels (pulmonary arteries) to the lungs. There, the blood releases carbon dioxide and picks up oxygen as it flows by the alveoli.
The oxygen-rich blood then returns to the left atrium through the pulmonary veins. It then flows through the mitral valve into the left ventricle. Finally, it leaves the heart through the body's main artery (aorta).
The heart valves keep blood flowing in the right direction. The aortic valve keeps the blood from flowing backward into the heart. From the aorta, the blood travels to the rest of the body.
Heart-related (cardiogenic) pulmonary edema
Cardiogenic pulmonary edema is caused by increased pressures in the heart.
It's usually a result of heart failure. When a diseased or overworked left lower heart chamber (left ventricle) can't pump out enough of the blood it gets from the lungs, pressures in the heart go up. The increased pressure pushes fluid through the blood vessel walls into the air sacs.
Medical conditions that can cause heart failure and lead to pulmonary edema include:
-
Coronary artery disease. Over time, the arteries that supply blood to the heart muscle can become narrow from fatty deposits (plaques). A slow narrowing of the coronary arteries can weaken the left ventricle.
Sometimes, a blood clot forms in one of these narrowed arteries. The clot blocks blood flow and damages part of the heart muscle, resulting in a heart attack. A damaged heart muscle can no longer pump as well as it should.
- Cardiomyopathy. This term means heart muscle damage. With cardiomyopathy, the heart must pump harder, and pressures rise. Then the heart might not be able to work harder when needed, such as during exercise or with an infection or a rise in blood pressure. When the left ventricle can't keep up with the demands that are placed on it, fluid backs up into the lungs.
- Heart valve problems. Narrowing (stenosis) of the aortic or mitral heart valves or a valve that leaks or doesn't close properly affects blood flow into the heart. A valve leak that develops suddenly might cause sudden and severe pulmonary edema.
- High blood pressure (hypertension). Untreated or uncontrolled high blood pressure can enlarge the heart.
- Other heart problems. Inflammation of the heart muscle (myocarditis), heart problems present at birth (congenital heart defects) and irregular heart rhythms (arrhythmias) also may cause pulmonary edema.
- Kidney disease. High blood pressure due to narrowed kidney arteries (renal artery stenosis) or fluid buildup due to kidney disease can cause pulmonary edema.
- Chronic health conditions. Thyroid disease and a buildup of iron (hemochromatosis) or protein (amyloidosis) also may contribute to heart failure and cause pulmonary edema.
Non-heart-related (noncardiogenic) pulmonary edema
Pulmonary edema that is not caused by increased pressures in the heart is called noncardiogenic pulmonary edema.
Causes of noncardiogenic pulmonary edema include:
- Acute respiratory distress syndrome (ARDS). This serious disorder occurs when the lungs suddenly fill with fluid. Many conditions can cause ARDS, including severe injury (trauma), widespread infection (sepsis), pneumonia and severe bleeding.
- Drug reaction or drug overdose. Many drugs — ranging from aspirin to illegal drugs such as heroin and cocaine — are known to cause pulmonary edema.
- Blood clot in the lungs (pulmonary embolism). A blood clot moving from the blood vessels in the legs to the lungs can cause pulmonary edema.
- Exposure to certain toxins. Inhaling toxins or breathing in some stomach contents when vomiting (aspiration) causes intense irritation of the small airways and air sacs, resulting in fluid buildup.
- High altitudes. Pulmonary edema has been seen in mountain climbers, skiers, hikers and other people who travel to high elevations, usually above 8,000 feet (about 2,400 meters). High-altitude pulmonary edema (HAPE) generally occurs in those who don't take the days or weeks needed to become used to the elevation. But people who live at high altitudes can get HAPE with no elevation change if they have a respiratory illness.
- Near drowning. Inhaling water causes fluid buildup in the lungs.
- Negative pressure pulmonary edema. A blocked upper airway causes negative pressure in the lungs from trying to breathe through the blockage. With treatment, most people with this type of pulmonary edema recover in about 24 hours.
- Nervous system conditions or surgeries. A type of pulmonary edema called neurogenic pulmonary edema can occur after a head injury, seizure or brain surgery.
- Smoke inhalation. Smoke from a fire contains chemicals that damage the membrane between the air sacs and the capillaries. The damage allows fluid to enter the lungs.
- Transfusion-related lung injury. Blood transfusions may cause fluid overload in the left ventricle, leading to pulmonary edema.
- Viral illnesses. Viruses such as the hantavirus and dengue virus can cause pulmonary edema.
Risk factors
Heart failure and other heart conditions that raise pressure in the heart increase the risk of pulmonary edema. Risk factors for heart failure include:
- Irregular heart rhythms (arrhythmias)
- Alcohol use
- Congenital heart disease
- Coronary artery disease
- Diabetes
- Heart valve disease
- High blood pressure
- Sleep apnea
Some nervous system conditions and lung damage due to near drowning, drug use, inhaling smoke, viral illnesses and blood clots also raise the risk.
People who travel to high-altitude locations above 8,000 feet (about 2,400 meters) are more likely to develop high-altitude pulmonary edema (HAPE). It usually affects those who don't take the time — a few days to a week or more — to get used to the elevation.
Children who already have pulmonary hypertension and structural heart defects may be more likely to get HAPE.
Complications
Complications of pulmonary edema depend on the cause.
In general, if pulmonary edema continues, the pressure in the pulmonary artery can rise (pulmonary hypertension). Eventually, the heart becomes weak and begins to fail, and pressures in the heart and lungs go up.
Pulmonary edema complications may include:
- Breathing difficulty
- Swelling of the legs, feet and belly area
- Buildup of fluid in the membranes that surround the lungs (pleural effusion)
- Congestion and swelling of the liver
Immediate treatment is necessary for acute pulmonary edema to prevent death.
Prevention
You may be able to prevent pulmonary edema by managing existing heart or lung conditions and following a healthy lifestyle.
For example, controlling cholesterol and blood pressure can help lower the risk of heart disease. Follow these tips to keep your heart healthy:
- Eat a healthy diet rich in fresh fruits, vegetables, whole grains, fat-free or low-fat dairy, and a variety of proteins.
- Don't smoke.
- Get regular exercise.
- Limit salt and alcohol.
- Manage stress.
- Manage weight.
Preventing high-altitude pulmonary edema (HAPE)
To prevent HAPE, gradually ascend to high elevations. Although recommendations vary, most experts advise increasing elevation no more than 1,000 to 1,200 feet (about 300 to 360 meters) a day once you reach 8,200 feet (about 2,500 meters).
Some climbers take prescription medications such as acetazolamide or nifedipine (Procardia) to help prevent symptoms of HAPE. To prevent HAPE, start taking the medication at least one day before ascent. Ask your health care provider how long you need to take the medication after you've arrived at your high-altitude destination.
Diagnosis
Breathing problems require immediate diagnosis and treatment. A health care provider can base a diagnosis of pulmonary edema on the symptoms and the results of a physical exam and certain tests.
Once the condition is more stable, the provider can ask about medical history, especially a history of cardiovascular or lung disease.
Tests that can help diagnose pulmonary edema or determine the reason for fluid in the lungs include:
- Chest X-ray. A chest X-ray can confirm the diagnosis of pulmonary edema and exclude other possible causes of shortness of breath. It's usually the first test done when a health care provider suspects pulmonary edema.
- Chest computerized tomography (CT) scan. A chest CT scan gives more details about the condition of the lungs. It can help a provider diagnose or rule out pulmonary edema.
- Pulse oximetry. A sensor is attached to a finger or ear. It uses light to determine how much oxygen is in the blood.
- Arterial blood gas test. This test measures the amount of oxygen and carbon dioxide in the blood.
- B-type natriuretic peptide (BNP) blood test. Increased levels of BNP may signal a heart condition.
- Other blood tests. Blood tests to diagnose pulmonary edema and its causes also usually include a complete blood count, metabolic panel to check kidney function and thyroid function test.
- Electrocardiogram (ECG or EKG). This painless test detects and records the timing and strength of the heart's signals. It uses small sensors (electrodes) attached to the chest and sometimes to the arms or legs. Wires attach the sensors to a machine, which displays or prints results. An ECG can show signs of heart wall thickening or previous heart attack. A portable ECG device such as a Holter monitor may be used to continuously monitor the heartbeat at home.
- Echocardiogram. An echocardiogram uses sound waves (ultrasound) to create pictures of the beating heart. It can identify areas of poor blood flow, heart valve issues and heart muscle that is not working properly. An echocardiogram can help diagnose fluid around the heart (pericardial effusion).
- Cardiac catheterization and coronary angiogram. This test may be done if other tests don't show the cause of pulmonary edema, or when there's also chest pain. It helps health care providers see blockages in the heart arteries. A long, flexible tube (catheter) is inserted in a blood vessel, usually in the groin or wrist. It's guided to the heart. Dye flows through the catheter to arteries in the heart. The dye helps the arteries show up more clearly on X-ray images and video.
- Ultrasound of the lungs. This painless test uses sound waves to measure blood flow through the lungs. It can quickly reveal signs of fluid buildup and plural effusions.
Treatment
The first treatment for acute pulmonary edema is oxygen. Oxygen flows through a face mask or a flexible plastic tube with two openings (nasal cannula) that deliver oxygen to each nostril. This should ease some symptoms.
A health care provider monitors the oxygen level. Sometimes it may be necessary to assist breathing with a machine such as a mechanical ventilator or one that provides positive airway pressure.
Depending on the severity of the condition and the reason for the pulmonary edema, treatment might include one or more of the following medications:
- Diuretics. Diuretics, such as furosemide (Lasix), decrease the pressure caused by excess fluid in the heart and lungs.
- Blood pressure drugs. These help manage high or low blood pressure, which can occur with pulmonary edema. A provider may also prescribe medications that lower the pressure going into or out of the heart. Examples of such medicines are nitroglycerin (Nitromist, Nitrostat, others) and nitroprusside (Nitropress).
- Inotropes. This type of medication is given through an IV for people in the hospital with severe heart failure. Inotropes improve heart pumping function and maintain blood pressure.
- Morphine (MS Contin, Infumorph, others). This narcotic may be taken by mouth or given through an IV to relieve shortness of breath and anxiety. But some care providers believe that the risks of morphine may outweigh the benefits. They're more likely to use other drugs.
It is important to diagnosis and treat, if possible, any nervous system problems or causes of heart failure.
Treating high-altitude pulmonary edema (HAPE)
Oxygen is the usually the first treatment. If oxygen isn't available, a portable hyperbaric chamber can imitate going down to a lower elevation until it's possible to move to a lower elevation.
Treatments for high-altitude pulmonary edema (HAPE) also include:
- Immediately going down to a lower elevation. For someone in high altitudes who has mild symptoms of HAPE, going down 1,000 to 3,000 feet (about 300 to 1,000 meters) as quickly as possible can help. Someone with severe HAPE might need rescue assistance to get off the mountain.
- Stopping exercise and staying warm. Physical activity and cold can make pulmonary edema worse.
- Medication. Some climbers take prescription medications such as acetazolamide or nifedipine (Procardia) to help treat or prevent symptoms of HAPE. To prevent HAPE, they start taking the medication at least a day before going higher.
Self care
Lifestyle changes are an important part of heart health and can help with some forms of pulmonary edema.
- Keep blood pressure under control. For high blood pressure, take medications as prescribed and check blood pressure regularly. Record the results. A health care provider can help set a target blood pressure.
- Manage other medical conditions. Address underlying medical conditions. For example, controlling glucose levels if you have diabetes.
- Avoid the cause of your condition. If pulmonary edema results from drug use or high altitudes, for example, avoiding using drugs or being in high altitudes can help prevent more lung damage.
- Don't smoke. It's always a healthy idea to stop smoking. For help with quitting, talk to a health care provider.
- Eat less salt. Salt helps the body retain fluid. In some people with damage in the left ventricle of the heart, too much salt might trigger congestive heart failure. A dietician can help with cutting salt by showing how to determine the salt content in foods and create a nutritious, good-tasting diet. In general, most people should consume less than 2,300 milligrams a day of salt (sodium). Ask your care provider what level is safe for you.
- Choose a healthy diet. A healthy diet includes plenty of fruits, vegetables and whole grains. Limit saturated fats and trans fats, added sugars, and sodium.
- Manage weight. Being even slightly overweight increases the risk of cardiovascular disease. But losing even small amounts of weight can lower blood pressure and cholesterol and reduce the risk of diabetes.
- Get regular exercise. Healthy adults should get at least 150 minutes of moderate aerobic activity or 75 minutes of vigorous aerobic activity a week, or a combination of the two. If you're not used to exercise, start out slowly and build up gradually. Be sure to get your care provider's OK before starting an exercise program.
Preparing for your appointment
If you have pulmonary edema, you will likely first be seen by an emergency room doctor. If you think you have signs or symptoms of pulmonary edema, call 911 or emergency medical help rather than making an outpatient appointment.
You may see several specialists while you're in the hospital. After you are stable, you may be referred to a doctor trained in heart conditions (cardiologist) or lung conditions (pulmonologist).
What you can do
- Write down your symptoms, including any that may seem unrelated to the reason for which you scheduled the appointment, and when they began.
- Write down if you have had similar symptoms in the past, even if you didn't see a health care provider.
- Write down key personal information, including any major stresses or recent life changes.
- Get copies of your medical records whenever possible. Discharge information from the hospital and results from heart tests, as well as letters from specialists you've seen can be helpful.
- Make a list of all medications as well as any vitamins or supplements you take, including doses.
- Keep written track of your weight and give that record to your care provider to look for trends.
- Make a list of the salty foods you eat regularly. Mention if you have eaten more of these recently.
- Ask a family member or friend to come along, if possible, to help you remember the information you're given.
- Write down questions to ask your care provider.
For pulmonary edema, some questions to ask include:
- What's the most likely cause of my symptoms?
- What tests do I need? Do these tests require any special preparation?
- What treatments are available, and which do you recommend?
- What types of side effects can I expect from treatment?
- Are there alternatives to the treatment you're suggesting?
- What's my prognosis?
- Are there dietary or activity restrictions that I need to follow? Would it help me to see a dietitian?
- Are there any brochures or other printed material that I can have? What websites do you recommend?
Don't hesitate to ask other questions.
What to expect from your doctor
Your provider is likely to ask you a number of questions, including:
- Have your symptoms been continuous?
- How severe are your symptoms? Have your symptoms affected your work or daily activities?
- Does anything seem to improve your symptoms?
- What, if anything, appears to make your symptoms worse?
- Have you been diagnosed with obstructive sleep apnea or do you have symptoms of obstructive sleep apnea?
- Do you have any family history of lung or heart disease?
- Have you ever been diagnosed with chronic obstructive pulmonary disease (COPD) or asthma?
- Do you smoke or did you smoke in the past? If so, how many packs a day and when did you quit?
- Do you travel to altitudes higher than 1 mile?

