
Barrett's esophagus
Overview
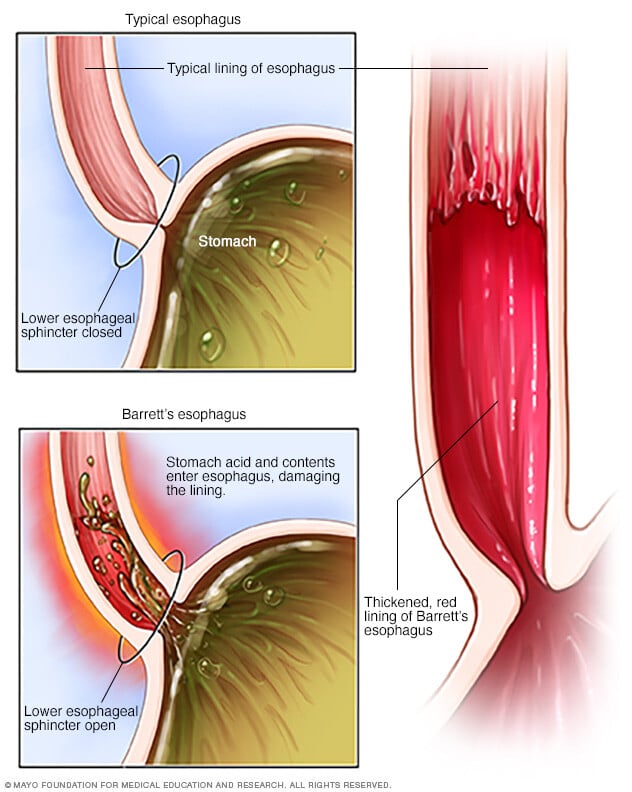
Barrett's esophagus is a condition in which the flat pink lining of the swallowing tube that connects the mouth to the stomach (esophagus) becomes damaged by acid reflux, which causes the lining to thicken and become red.
Between the esophagus and the stomach is a critically important valve, the lower esophageal sphincter (LES). Over time, the LES may begin to fail, leading to acid and chemical damage of the esophagus, a condition called gastroesophageal reflux disease (GERD). GERD is often accompanied by symptoms such as heartburn or regurgitation. In some people, this GERD may trigger a change in the cells lining the lower esophagus, causing Barrett's esophagus.
Barrett's esophagus is associated with an increased risk of developing esophageal cancer. Although the risk of developing esophageal cancer is small, it's important to have regular checkups with careful imaging and extensive biopsies of the esophagus to check for precancerous cells (dysplasia). If precancerous cells are discovered, they can be treated to prevent esophageal cancer.
Symptoms
The development of Barrett's esophagus is most often attributed to long-standing GERD, which may include these signs and symptoms:
- Frequent heartburn and regurgitation of stomach contents
- Difficulty swallowing food
- Less commonly, chest pain
Curiously, approximately half of the people diagnosed with Barrett's esophagus report little if any symptoms of acid reflux. So, you should discuss your digestive health with your doctor regarding the possibility of Barrett's esophagus.
When to see a doctor
If you've had trouble with heartburn, regurgitation and acid reflux for more than five years, then you should ask your doctor about your risk of Barrett's esophagus.
Seek immediate help if you:
- Have chest pain, which may be a symptom of a heart attack
- Have difficulty swallowing
- Are vomiting red blood or blood that looks like coffee grounds
- Are passing black, tarry or bloody stools
- Are unintentionally losing weight
Causes
The exact cause of Barrett's esophagus isn't known. While many people with Barrett's esophagus have long-standing GERD, many have no reflux symptoms, a condition often called "silent reflux."
Whether this acid reflux is accompanied by GERD symptoms or not, stomach acid and chemicals wash back into the esophagus, damaging esophagus tissue and triggering changes to the lining of the swallowing tube, causing Barrett's esophagus.
Risk factors
Factors that increase your risk of Barrett's esophagus include:
- Family history. Your odds of having Barrett's esophagus increase if you have a family history of Barrett's esophagus or esophageal cancer.
- Being male. Men are far more likely to develop Barrett's esophagus.
- Being white. White people have a greater risk of the disease than do people of other races.
- Age. Barrett's esophagus can occur at any age but is more common in adults over 50.
- Chronic heartburn and acid reflux. Having GERD that doesn't get better when taking medications known as proton pump inhibitors or having GERD that requires regular medication can increase the risk of Barrett's esophagus.
- Current or past smoking.
- Being overweight. Body fat around your abdomen further increases your risk.
Complications
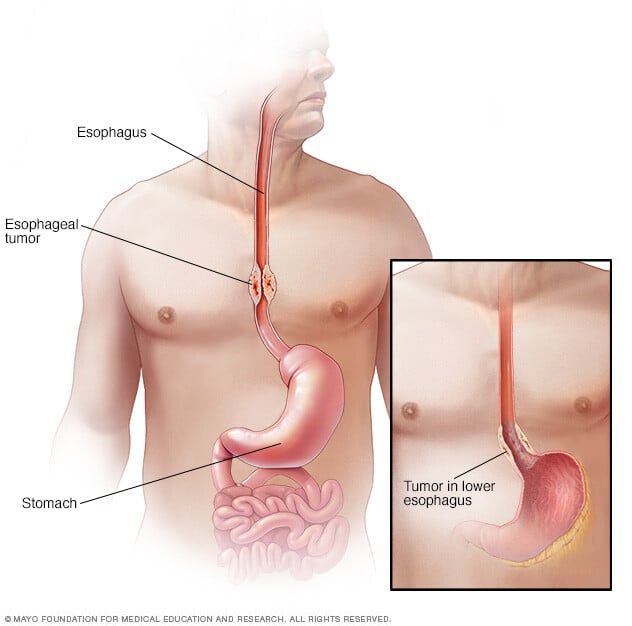
People with Barrett's esophagus have an increased risk of esophageal cancer. The risk is small, even in people who have precancerous changes in their esophagus cells. Fortunately, most people with Barrett's esophagus will never develop esophageal cancer.
Diagnosis
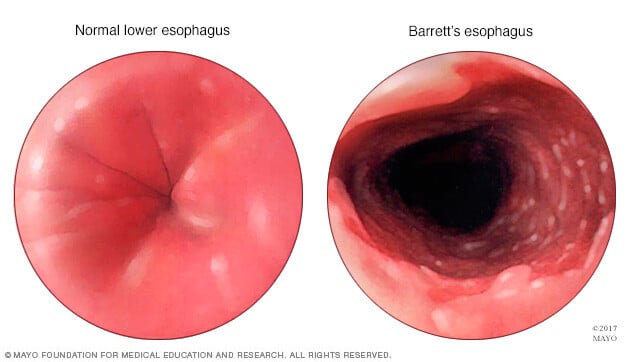
Endoscopy is generally used to determine if you have Barrett's esophagus.
A lighted tube with a camera at the end (endoscope) is passed down your throat to check for signs of changing esophagus tissue. Normal esophagus tissue appears pale and glossy. In Barrett's esophagus, the tissue appears red and velvety.
Your doctor will remove tissue (biopsy) from your esophagus. The biopsied tissue can be examined to determine the degree of change.
Determining the degree of tissue change
A doctor who specializes in examining tissue in a laboratory (pathologist) determines the degree of dysplasia in your esophagus cells. Because it can be difficult to diagnose dysplasia in the esophagus, it's best to have two pathologists — with at least one who specializes in gastroenterology pathology — agree on your diagnosis. Your tissue may be classified as:
- No dysplasia, if Barrett's esophagus is present but no precancerous changes are found in the cells.
- Low-grade dysplasia, if cells show small signs of precancerous changes.
- High-grade dysplasia, if cells show many changes. High-grade dysplasia is thought to be the final step before cells change into esophageal cancer.
Screening for Barrett's esophagus
The American College of Gastroenterology says screening may be recommended for men who have had GERD symptoms at least weekly that don't respond to treatment with proton pump inhibitor medication, and who have at least two more risk factors, including:
- Having a family history of Barrett's esophagus or esophageal cancer
- Being male
- Being white
- Being over 50
- Being a current or past smoker
- Having a lot of abdominal fat
While women are significantly less likely to have Barrett's esophagus, women should be screened if they have uncontrolled reflux or have other risk factors for Barrett's esophagus.
Treatment
Treatment for Barrett's esophagus depends on the extent of abnormal cell growth in your esophagus and your overall health.
No dysplasia
Your doctor will likely recommend:
- Periodic endoscopy to monitor the cells in your esophagus. If your biopsies show no dysplasia, you'll probably have a follow-up endoscopy in one year and then every three to five years if no changes occur.
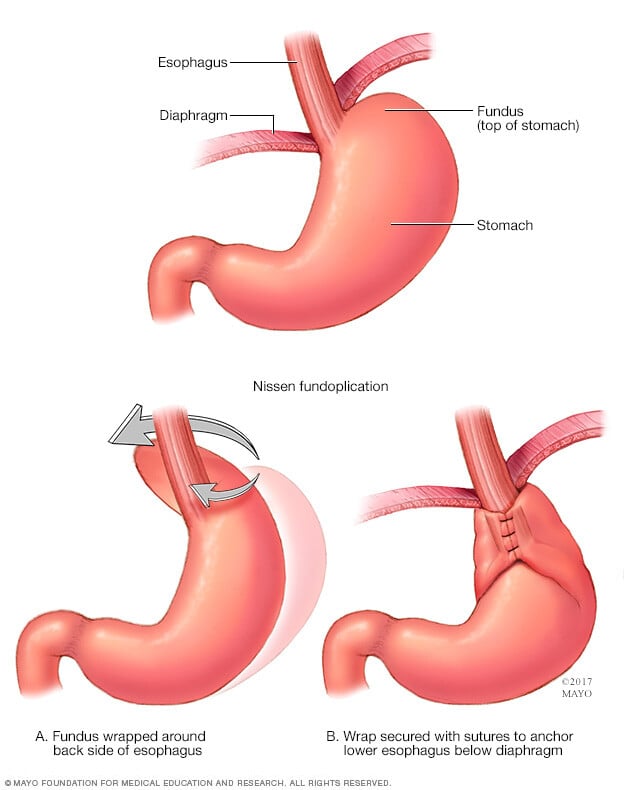
- Treatment for GERD. Medication and lifestyle changes can ease your signs and symptoms. Surgery or endoscopy procedures to correct a hiatal hernia or to tighten the lower esophageal sphincter that controls the flow of stomach acid may be an option.
Low-grade dysplasia
Low-grade dysplasia is considered the early stage of precancerous changes. If low-grade dysplasia is found, it should be verified by an experienced pathologist. For low-grade dysplasia, your doctor may recommend another endoscopy in six months, with additional follow-up every six to 12 months.
But, given the risk of esophageal cancer, treatment may be recommended if the diagnosis is confirmed. Preferred treatments include:
- Endoscopic resection, which uses an endoscope to remove damaged cells to aid in the detection of dysplasia and cancer.
- Radiofrequency ablation, which uses heat to remove abnormal esophagus tissue. Radiofrequency ablation may be recommended after endoscopic resection.
- Cryotherapy, which uses an endoscope to apply a cold liquid or gas to abnormal cells in the esophagus. The cells are allowed to warm up and then are frozen again. The cycle of freezing and thawing damages the abnormal cells.
If significant inflammation of the esophagus is present at initial endoscopy, another endoscopy is performed after you've received three to four months of treatment to reduce stomach acid.
High-grade dysplasia
High-grade dysplasia is generally thought to be a precursor to esophageal cancer. For this reason, your doctor may recommend endoscopic resection, radiofrequency ablation or cryotherapy. Another option may be surgery, which involves removing the damaged part of your esophagus and attaching the remaining portion to your stomach.
Recurrence of Barrett's esophagus is possible after treatment. Ask your doctor how often you need to come back for follow-up testing. If you have treatment other than surgery to remove abnormal esophageal tissue, your doctor is likely to recommend lifelong medication to reduce acid and help your esophagus heal.
Lifestyle and home remedies
Lifestyle changes can ease symptoms of GERD, which may underlie Barrett's esophagus. Consider:
- Maintaining a healthy weight.
- Eliminating foods and drinks that trigger your heartburn, such as chocolate, coffee, alcohol and mint.
- Stopping smoking.
- Raising the head of your bed. Place wooden blocks under your bed to elevate your head.
Preparing for an appointment
Barrett's esophagus is most often diagnosed in people with GERD who are being examined for GERD complications. If your doctor discovers Barrett's esophagus on an endoscopy exam, you may be referred to a doctor who treats digestive diseases (gastroenterologist).
What you can do
- Be aware of any pre-appointment restrictions, such as not eating solid food on the day before your appointment.
- Write down your symptoms, including any that may seem unrelated to the reason why you scheduled the appointment.
- Make a list of all your medications, vitamins and supplements.
- Write down your key medical information, including other conditions.
- Ask a relative or friend to accompany you to help you remember what the doctor says.
- Write down questions to ask your doctor.
Questions to ask your doctor
- Do my lab reports show precancerous changes (dysplasia)? If so, what is the grade of my dysplasia?
- How much of my esophagus is affected?
- How often should I be screened for changes to my esophagus?
- Do I have dysplasia and if so was it confirmed by an expert pathologist?
- What's my risk of esophageal cancer?
- What are the treatment options?
- Do I need to make diet or other lifestyle changes?
- I have other health conditions. How can I best manage these conditions together?
In addition to the questions that you've prepared to ask your doctor, don't hesitate to ask additional questions during your appointment.
What to expect from your doctor
Your doctor is likely to ask you a number of questions. Being ready to answer them may make time to go over points you want to spend more time on. You may be asked:
- When did you first begin experiencing symptoms? How severe are they?
- Are your symptoms continuous or occasional?
- What, if anything, seems to worsen your symptoms? Does anything make your symptoms better?
- Do you experience acid reflux symptoms?
- Do you take any medications for reflux or indigestion?
- Do you have difficulty swallowing?
- Have you lost weight?

