
Myelofibrosis
Overview
Myelofibrosis is an uncommon type of bone marrow cancer that disrupts your body's normal production of blood cells.
Myelofibrosis causes extensive scarring in your bone marrow, leading to severe anemia that can cause weakness and fatigue. Bone marrow scarring can also cause you to have a low number of blood-clotting cells called platelets, which increases the risk of bleeding. Myelofibrosis often causes an enlarged spleen.
Myelofibrosis is considered to be a chronic leukemia — a cancer that affects the blood-forming tissues in the body. Myelofibrosis belongs to a group of diseases called myeloproliferative disorders.
Myelofibrosis can happen on its own (primary myelofibrosis) or it can develop from another bone marrow disorder (secondary myelofibrosis).
Some people with myelofibrosis have no symptoms and might not need treatment right away. Others with more-serious forms of the disease might need aggressive treatments right away. Treatment for myelofibrosis, which focuses on relieving symptoms, can involve a variety of options.
Symptoms
Myelofibrosis usually develops slowly. In its very early stages, many people don't experience signs or symptoms.
As disruption of normal blood cell production increases, signs and symptoms may include:
- Feeling tired, weak or short of breath, usually because of anemia
- Pain or fullness below your ribs on the left side, due to an enlarged spleen
- Easy bruising
- Easy bleeding
- Excessive sweating during sleep (night sweats)
- Fever
- Bone pain
When to see a doctor
Make an appointment with your doctor if you have any persistent signs and symptoms that worry you.
Causes
Myelofibrosis occurs when bone marrow stem cells develop changes (mutations) in their DNA. The stem cells have the ability to replicate and divide into the multiple specialized cells that make up your blood — red blood cells, white blood cells and platelets.
It's not clear what causes the genetic mutations in bone marrow stem cells.
As the mutated blood stem cells replicate and divide, they pass along the mutations to the new cells. As more and more of these mutated cells are created, they begin to have serious effects on blood production.
The end result is usually a lack of red blood cells — which causes the anemia characteristic of myelofibrosis — and an overabundance of white blood cells and varying levels of platelets. In people with myelofibrosis, the normally spongy bone marrow becomes scarred.
Several specific gene mutations have been identified in people with myelofibrosis. The most common is the Janus kinase 2 (JAK2) gene mutation. Other less common mutations include CALR and MPL. Some people with myelofibrosis don't have any identifiable gene mutations. Knowing whether these gene mutations are associated with your myelofibrosis helps determine your prognosis and your treatment.
Risk factors
Although the cause of myelofibrosis often isn't known, certain factors are known to increase your risk:
- Age. Myelofibrosis can affect anyone, but it's most often diagnosed in people older than 50.
- Another blood cell disorder. A small portion of people with myelofibrosis develop the condition as a complication of essential thrombocythemia or polycythemia vera.
- Exposure to certain chemicals. Myelofibrosis has been linked to exposure to industrial chemicals such as toluene and benzene.
- Exposure to radiation. People exposed to very high levels of radiation have an increased risk of myelofibrosis.
Complications
Complications that may result from myelofibrosis include:
- Increased pressure on blood flowing into your liver. Normally, blood flow from the spleen enters your liver through a large blood vessel called the portal vein. Increased blood flow from an enlarged spleen can lead to high blood pressure in the portal vein (portal hypertension). This in turn can force excess blood into smaller veins in your stomach and esophagus, potentially causing these veins to rupture and bleed.
- Pain. A severely enlarged spleen can cause abdominal pain and back pain.
- Growths in other areas of your body. Formation of blood cells outside the bone marrow (extramedullary hematopoiesis) may create clumps (tumors) of developing blood cells in other areas of your body. These tumors may cause problems such as bleeding in your gastrointestinal system, coughing or spitting up of blood, compression of your spinal cord, or seizures.
- Bleeding complications. As the disease progresses, your platelet count tends to drop below normal (thrombocytopenia) and platelet function becomes impaired. An insufficient number of platelets can lead to easy bleeding — an issue that you and your doctor will want to discuss if you're contemplating any type of surgical procedure.
- Acute leukemia. Some people with myelofibrosis eventually develop acute myelogenous leukemia, a type of blood and bone marrow cancer that progresses rapidly.
Diagnosis
Tests and procedures used to diagnose myelofibrosis include:
- Physical exam. Your doctor will perform a physical exam. This includes a check of vital signs, such as pulse and blood pressure, as well as checks of your lymph nodes, spleen and abdomen.
- Blood tests. In myelofibrosis, a complete blood count typically shows abnormally low levels of red blood cells, a sign of anemia common in people with myelofibrosis. White blood cell and platelet counts are usually abnormal, too. Often, white blood cell levels are higher than normal, although in some people they may be normal or even lower than normal. Platelet counts may be higher or lower than normal.
- Imaging tests. Imaging tests, such as X-rays and MRI, may be used to gather more information about your myelofibrosis.
-
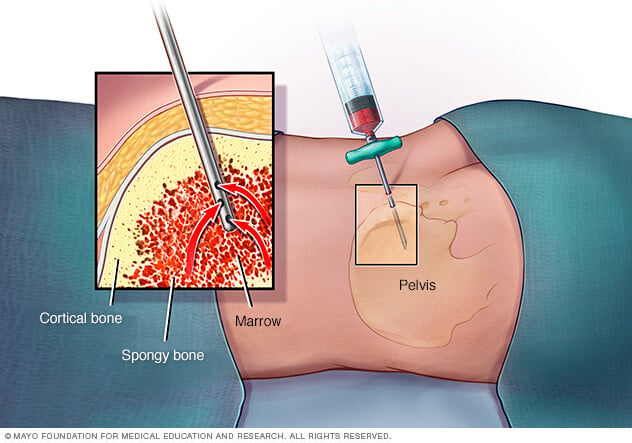
Bone marrow examination. Bone marrow biopsy and aspiration can confirm a diagnosis of myelofibrosis.
In a bone marrow biopsy, a needle is used to draw a sample of bone tissue and the enclosed marrow from your hipbone. During the same procedure, another type of needle may be used to withdraw a sample of the liquid portion of your bone marrow. The samples are studied in a laboratory to determine the numbers and types of cells found.
- Testing cancer cells for gene mutations. In a laboratory, doctors will analyze your blood or bone marrow cells for gene mutations, such as JAK2, CALR and MPL. Your doctor uses the information from these tests to determine your prognosis and your treatment options.
Treatment
The goal of treatment for most people with myelofibrosis is to provide relief from signs and symptoms of the disease. For some, a bone marrow transplant may provide a chance for a cure, but this treatment is very hard on the body and it might not be an option for many people.
In order to determine which myelofibrosis treatments are most likely to benefit you, your doctor may use one or more formulas to assess your condition. These formulas take into account many aspects of your cancer and your overall health to assign a risk category that indicates the aggressiveness of the disease.
Low-risk myelofibrosis may not require immediate treatment, while people with high-risk myelofibrosis may consider an aggressive treatment, such as bone marrow transplant. For intermediate-risk myelofibrosis, treatment is usually directed at managing symptoms.
Immediate treatment may not be necessary
Myelofibrosis treatment may not be necessary if you aren't experiencing symptoms. You might not need treatment right away if you don't have an enlarged spleen and you don't have anemia or your anemia is very mild. Rather than treatment, your doctor is likely to monitor your health closely through regular checkups and exams, watching for any signs of disease progression. Some people remain symptom-free for years.
Treatments for anemia
If myelofibrosis is causing severe anemia, you may consider treatment, such as:
- Blood transfusions. If you have severe anemia, periodic blood transfusions can increase your red blood cell count and ease anemia symptoms, such as fatigue and weakness. Sometimes, medications can help improve anemia.
- Androgen therapy. Taking a synthetic version of the male hormone androgen may promote red blood cell production and may improve severe anemia in some people. Androgen therapy does have risks, including liver damage and masculinizing effects in women.
- Thalidomide and related medications. Thalidomide (Thalomid) and the related drug lenalidomide (Revlimid) may help improve blood cell counts and may also relieve an enlarged spleen. These drugs may be combined with steroid medications. Thalidomide and related drugs carry a risk of serious birth defects and require special precautions.
Treatments for an enlarged spleen
If an enlarged spleen is causing complications, your doctor may recommend treatment. Your options may include:
- Targeted drug therapy. Targeted drug treatments focus on specific abnormalities present within cancer cells. Targeted treatments for myelofibrosis focus on cells with the JAK2 gene mutation. These treatments are used to reduce symptoms of an enlarged spleen.
- Chemotherapy. Chemotherapy uses powerful drugs to kill cancer cells. Chemotherapy drugs may reduce the size of an enlarged spleen and relieve related symptoms, such as pain.
-
Surgical removal of the spleen (splenectomy). If your spleen becomes so large that it causes you pain and begins to cause harmful complications — and if you don't respond to other forms of therapy — you may benefit from having your spleen surgically removed.
Risks include infection, excessive bleeding and blood clot formation leading to stroke or pulmonary embolism. After the procedure, some people experience liver enlargement and an abnormal increase in platelet count.
- Radiation therapy. Radiation uses high-powered beams, such as X-rays and protons, to kill cancer cells. Radiation therapy can help reduce the size of the spleen when surgical removal isn't an option.
Bone marrow transplant
A bone marrow transplant, also called a stem cell transplant, is a procedure to replace your diseased bone marrow using healthy blood stem cells. For myelofibrosis, the procedure uses stem cells from a donor (allogeneic stem cell transplant).
This treatment has the potential to cure myelofibrosis, but it also carries a high risk of life-threatening side effects, including a risk that the new stem cells will react against your body's healthy tissues (graft-versus-host disease).
Many people with myelofibrosis, because of age, stability of the disease or other health problems, don't qualify for this treatment.
Prior to a bone marrow transplant, you receive chemotherapy or radiation therapy to destroy your diseased bone marrow. Then you receive infusions of stem cells from a compatible donor.
Supportive (palliative) care
Palliative care is specialized medical care that focuses on providing relief from pain and other symptoms of a serious illness. Palliative care specialists work with you, your family and your other doctors to provide an extra layer of support that complements your ongoing care. Palliative care can be used while undergoing other aggressive treatments, such as surgery, chemotherapy or radiation therapy.
When palliative care is used along with all of the other appropriate treatments, people with cancer may feel better and live longer.
Palliative care is provided by a team of doctors, nurses and other specially trained professionals. Palliative care teams aim to improve the quality of life for people with cancer and their families. This form of care is offered alongside curative or other treatments you may be receiving.
Coping and support
Living with myelofibrosis may involve coping with pain, discomfort, uncertainty and the side effects of long-term treatments. The following steps may help ease the challenge and make you feel more comfortable and in charge of your health:
- Learn enough about your condition to feel comfortable making decisions. Myelofibrosis is fairly uncommon. To help you find accurate and trustworthy information, ask your doctor to direct you toward appropriate sources. Using these sources, find out as much as you can about myelofibrosis.
-
Get support. Take this opportunity to lean on family and friends. It can be tough to talk about your diagnosis, and you'll likely get a range of reactions when you share the news. But talking about your diagnosis and passing along information about your condition can help you build a support network. So can the offers of help that often result.
You may also benefit from joining a support group, either in your community or on the internet. A support group of people with the same or a similar diagnosis, such as a myeloproliferative disorder or another rare disease, can be a source of useful information, practical tips and encouragement.
-
Explore ways to cope with the disease. If you have myelofibrosis, you may face frequent bloodwork and medical appointments and regular bone marrow exams. Some days, you may feel sick even if you don't look sick. And some days, you may just be sick of being sick.
Try to find an activity that helps, whether it's yoga, exercise, socializing or adopting a more flexible work schedule. Talk to a counselor, therapist or oncology social worker if you need help dealing with the emotional challenges of this disease.
Preparing for an appointment
If your primary doctor suspects that you have myelofibrosis — often based on an enlarged spleen and abnormal blood tests — you're likely to be referred to a doctor who specializes in blood disorders (hematologist).
Because appointments can be brief, and because there's often a lot of information to discuss, it's a good idea to be prepared. Here's some information to help you get ready, and what to expect from your doctor.
What you can do
- Be aware of any pre-appointment restrictions. At the time you make the appointment, be sure to ask if there's anything you need to do in advance, such as restrict your diet.
- Write down any symptoms you're experiencing, including any that may seem unrelated to the reason for which you scheduled the appointment.
- Write down key personal information, including any major stresses or recent life changes.
- Make a list of all medications, vitamins or supplements that you're taking.
- Take a family member or friend along. Sometimes it can be difficult to remember all the information provided during an appointment. Someone who accompanies you may remember something that you missed or forgot.
- Write down questions to ask your doctor.
Your time with your doctor is limited, so preparing a list of questions will help you make the most of your time together. List your questions from most important to least important in case time runs out. For myelofibrosis, some basic questions to ask your doctor include:
- What is likely causing my symptoms or condition?
- What are other possible causes for my symptoms or condition?
- What kinds of tests do I need?
- Is my condition likely temporary or chronic?
- What is the best course of action?
- What are the alternatives to the primary approach that you're suggesting?
- I have other health conditions. How can I best manage them together?
- Are there any restrictions that I need to follow?
- Should I see a specialist? What will that cost, and will my insurance cover it?
- Is there a generic alternative to the medicine you're prescribing?
- Are there any brochures or other printed material that I can take with me? What websites do you recommend?
- What will determine whether I should plan for a follow-up visit?
In addition to the questions that you've prepared to ask your doctor, don't hesitate to ask additional questions during your appointment.
What to expect from your doctor
Your doctor is likely to ask you a number of questions. Being ready to answer them may allow more time to cover other points you want to address. Your doctor may ask:
- When did you first begin experiencing symptoms?
- Have your symptoms been continuous or occasional?
- How severe are your symptoms?
- What, if anything, seems to improve your symptoms?
- What, if anything, appears to worsen your symptoms?

