
Infertility
Overview
If you and your partner are struggling to have a baby, you're not alone. Millions of people around the world face the same challenge. Infertility is the medical term for when you can't get pregnant despite having frequent, unprotected sex for at least a year for most couples.
Infertility may happen because of a health issue with either you or your partner, or a mix of factors that prevent pregnancy. But many safe and effective treatments can boost your chances of getting pregnant.
Symptoms
The main symptom of infertility is not getting pregnant. There may be no other clear symptoms. Some women with infertility may have irregular menstrual periods or no periods. And some men may have some symptoms of hormonal problems, such as changes in hair growth or sexual function.
Many couples eventually will conceive — with or without treatment.
When to see a doctor
You likely don't need to see a member of your healthcare team about infertility unless you've been trying to get pregnant for at least one year. But women should talk with a healthcare professional sooner if they:
- Are age 35 or older and have tried to conceive for six months or longer.
- Are over age 40.
- Have no periods, or irregular or very painful periods.
- Have known fertility problems.
- Have endometriosis or a history of pelvic inflammatory disease.
- Have had more than one miscarriage.
- Have gotten cancer treatment such as chemotherapy or radiation.
Men should talk to a healthcare professional if they have:
- A low number of sperm or other problems with sperm.
- A history of testicular, prostate or sexual conditions.
- Had treatment for cancer such as chemotherapy.
- Had hernia surgery.
- Testicles that are smaller than the typical adult size, or swollen veins in the bag of skin that holds the testicles, called the scrotum.
- Had infertility with a partner in the past.
- Relatives with infertility problems.
Causes
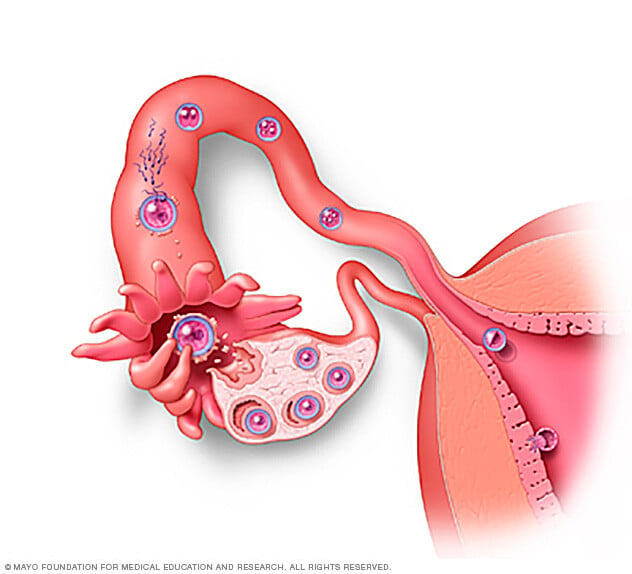
All of the steps during ovulation and fertilization need to happen correctly in order to get pregnant. Ovulation is the release of an egg from an ovary. Fertilization is when the egg and sperm unite to form an embryo, which becomes an unborn baby during pregnancy. Sometimes, the issues that cause infertility in couples are present at birth. Other times, they develop later in life.
Infertility causes can affect one or both partners. In some cases, no cause can be found.
Causes of male infertility
These can include:
- Conditions that can affect how much sperm is made or sperm quality. These medical conditions can include undescended testicles, genetic defects, hormone problems and health problems such as diabetes. Infections such as chlamydia, gonorrhea, mumps or HIV also can impact sperm. Enlarged veins in the scrotum, called a varicocele, can affect sperm's quality.
- Problems with sperm reaching the female reproductive tract. These issues can be due to sexual conditions such as premature ejaculation, certain genetic diseases such as cystic fibrosis, physical problems such as a blockage in the testicle, or damage or an injury to the reproductive organs.
- Certain factors in the environment. Exposure to pesticides, other chemicals or radiation can affect fertility. So can medicines that treat bacterial infections, high blood pressure and depression. And if the testicles often are exposed to heat, such as in saunas or hot tubs, that may affect their ability to make sperm.
- Damage related to cancer and its treatment. Cancer treatments such as chemotherapy and radiation can affect sperm production.
Causes of female infertility
These can include:
- Ovulation disorders. These conditions affect the release of eggs from the ovaries. They include hormonal problems such as polycystic ovary syndrome. High levels of a hormone needed to make breast milk, called prolactin, also may have an effect on ovulation. Either too much thyroid hormone, called hyperthyroidism, or too little, called hypothyroidism, can affect the menstrual cycle or cause infertility. Other underlying causes may include too much exercise, eating disorders or tumors.
- Conditions of the uterus. These include growths called uterine polyps, issues with the shape of the uterus or problems with its lower end, called the cervix. Tumors in the wall of the uterus, called uterine fibroids, also may cause infertility — but they aren't cancer. Fibroids can block the fallopian tubes, where an egg and sperm unite. They also can stop a fertilized egg from attaching to the uterus, which needs to happen for an unborn baby to develop.
- Fallopian tube damage or blockage. Often, these issues are caused by swelling of the fallopian tube, called salpingitis. The swelling can happen due to an infection of the female reproductive organs called pelvic inflammatory disease.
- Endometriosis. With this condition, tissue that's similar to the inner lining of the uterus grows outside of the uterus. It may affect the how well the ovaries, uterus and fallopian tubes work.
- Primary ovarian insufficiency. This happens when the ovaries stop working as they should, and menstrual periods end before age 40. The cause is often unknown. But some factors linked with primary ovarian insufficiency include immune system diseases, genetic conditions such as Turner syndrome, and radiation or chemotherapy treatment.
- Pelvic adhesions. These are bands of scar tissue that bind organs. They can form after a pelvic infection, appendicitis, endometriosis, or surgery of the abdomen or pelvis.
- Cancer and its treatment. Certain cancers — especially ones that affect the reproductive organs — often reduce female fertility. Both radiation and chemotherapy may affect fertility as well.
Risk factors
Many of the risk factors for both male and female infertility are the same. They include:
- Age. Women's fertility slowly declines with age, especially in the mid-30s. It drops quickly after age 37. Infertility in older women likely is due to the lower number and quality of eggs, or to health problems that affect fertility. Men over age 40 may be less fertile than younger men. The risk of birth defects and genetic problems also rises for children born to men over age 40.
- Tobacco use. Smoking tobacco by either partner may lower the chances of pregnancy. It also can make fertility treatments less effective. The risk of miscarriages may rise in women who smoke tobacco. When a pregnant person's partner smokes, that also raises the risk of miscarriage — even when the pregnant person is not a smoker. And smoking can raise the risk of erectile dysfunction and a low sperm count in men.
- Marijuana use. Marijuana may affect fertility, but more research is needed. Use during pregnancy has been linked with negative health effects on unborn babies. It also might raise the risk of miscarriage and stillbirth.
- Alcohol use. For women, there is no safe level of alcohol use when you're trying to get pregnant or during pregnancy. Alcohol may contribute to infertility. For men, heavy drinking can lower sperm count and affect how well sperm move.
- Being overweight. An inactive lifestyle and being overweight or obese can raise the risk of infertility. Obesity is linked with lower quality of semen, the fluid that contains sperm.
- Being underweight. People at risk of fertility problems include those with eating disorders, such as anorexia or bulimia. Those who follow a very low-calorie or restrictive diet also are at risk.
- Exercise issues. A lack of exercise plays a role in obesity, which raises the risk of infertility. Less often, ovulation problems may be linked with frequent, strenuous, intense exercise in women who are not overweight.
Prevention
Some types of infertility can't be prevented. But the following tips may boost your chances of pregnancy.
Couples
Have sex often soon after menstrual bleeding stops. One of the ovaries usually releases an egg in the middle of the cycle — halfway between menstrual periods — for most people with menstrual cycles about 28 days apart. It's ideal to have sex every day starting 5 to 7 days before the release of the egg. Continue until two days after ovulation.
Men
Most types of infertility aren't preventable in men, but these tips may help:
- Stay away from drugs and tobacco, and don't drink a lot of alcohol. Doing illegal drugs, smoking or drinking heavily can raise the risk of male infertility.
- Don't take frequent baths in hot water. The high temperatures can have a short-term effect on sperm production and movement.
- Stay away from pollutants and toxins. These include pesticides, lead, cadmium and mercury. Being exposed to them can affect the body's ability to make sperm.
- Limit medicines that may impact fertility if possible. Talk with your health care team about any medicines you take regularly. Don't stop any taking prescription drugs without medical advice.
- Work out. Regular exercise may improve sperm quality and boost the chances of a pregnancy.
Women
For women, the following tips may boost the chances of getting pregnant:
- Quit smoking. Tobacco has many bad effects on fertility. It's also terrible for your health and the health of an unborn baby. If you smoke and you want to try to become pregnant, quit tobacco now. You can ask your health care team for help.
- Stay away from alcohol and street drugs. These substances could make you less likely to conceive and have a healthy pregnancy. Don't drink alcohol or use recreational drugs, such as marijuana, if you're trying to get pregnant.
- Limit caffeine. Some women may need to cut back on caffeine when they try to get pregnant. Asks your health care team for advice. During pregnancy, many experts recommend you have no more than 200 milligrams of caffeine per day. That's about the amount in a 12-ounce cup of brewed coffee. Check food labels for amounts of caffeine too. The effects of caffeine aren't clear for an unborn baby. But the effects of higher amounts may include miscarriage or preterm birth.
- Exercise safely. Regular exercise is key for good health. But working out too intensely could cause your periods to happen less often or go away, and that could affect fertility.
- Get to a healthy weight. Being overweight or underweight can affect your hormones and cause infertility.
Diagnosis
Before infertility testing, your health care team or clinic works to understand your sexual habits. They might make recommendations to improve your chances of getting pregnant. But in some infertile couples, no clear cause is found. That is called unexplained infertility.
Infertility testing can involve uncomfortable procedures. It can be expensive too. And some medical plans may not cover the cost of fertility treatment. Also, there's no guarantee that you'll get pregnant — even after all the testing and counseling.
Tests for men
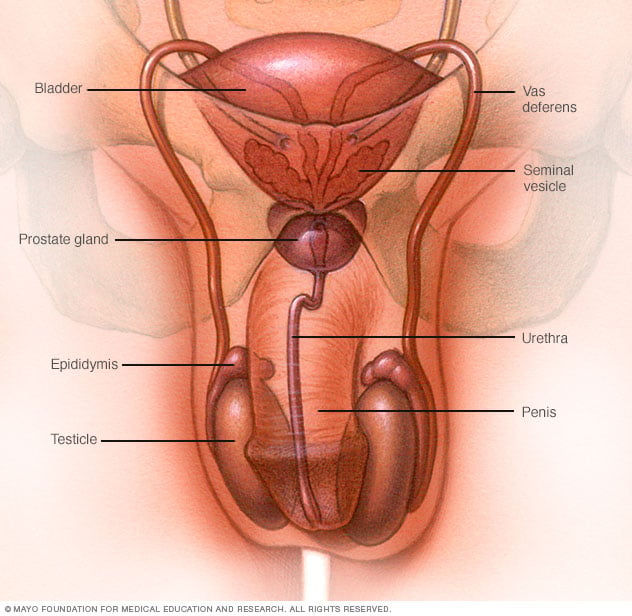
Male fertility relies on the testicles making enough healthy sperm. The sperm needs to be released from the penis into the vagina, where it has to travel to the waiting egg. Tests for male infertility try to find out whether there are treatable problems with any of these steps.
You may have a physical exam that includes a check of your genitals. Specific infertility tests may include:
- Semen analysis. Your health care team may ask for one or more samples of your semen. Often, you collect semen by masturbating or by stopping sex to ejaculate into a clean container. Then a lab checks your semen sample. In some cases, urine may be tested to find out if it contains sperm.
- Hormone testing. You may get a blood test to check your level of testosterone and other male hormones.
- Genetic testing. This may be done to find out whether a genetic defect is the cause of infertility.
- Testicular biopsy.This procedure removes a small amount of testicle tissue so a lab can check it under a microscope. It's not common to need a biopsy during infertility testing. Rarely, it may be done to find out whether there is a blockage in the reproductive tract that keeps sperm from leaving the body in semen. Most of the time, this diagnosis can be made based on your history, physical exam and lab tests. Other times, a biopsy may be done to find conditions that contribute to infertility. Or it may be used to collect sperm for assisted reproductive techniques, such as in vitro fertilization (IVF).
- Imaging. In some cases, your health care team may recommend tests that make pictures of the inside of your body. For example, ultrasound can check for problems in the scrotum, in the glands that make fluids that become semen or in the tube that carries sperm out of the testicles. A brain MRI can check for tumors of the pituitary gland that are not cancer. These tumors can cause the gland to make too much of the hormone prolactin, which could lead the body to make less sperm or none.
- Other testing. In rare cases, other tests may be done to check the quality of your sperm. For example, a semen sample may need to be checked for problems with DNA that might damage sperm.
Tests for women
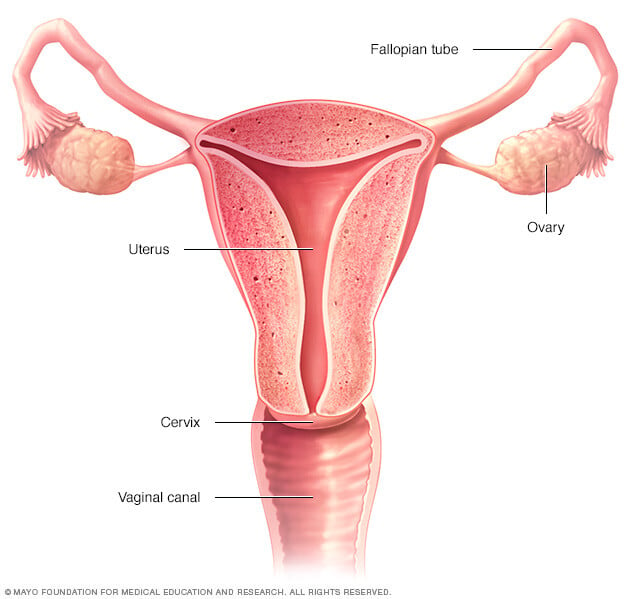
Fertility for women relies on the ovaries releasing healthy eggs. The reproductive tract must let an egg pass into the fallopian tubes and join with sperm. Then the fertilized egg must travel to the uterus and attach to the lining. Tests for female infertility try to find problems with any of those steps.
You may have a physical exam, including a regular pelvic exam. Infertility tests may include:
- Ovulation testing. A blood test measures hormone levels to find out whether you're ovulating.
- Thyroid function test. This blood test can be done if your health care team thinks your infertility might be related to a problem with the thyroid gland. If the gland makes too much or little thyroid hormone, that could play a role in fertility trouble.
- Hysterosalpingography. Hysterosalpingography (his-tur-o-sal-ping-GOG-ruh-fee) checks on the condition of the uterus and fallopian tubes. It also looks for blockages in the fallopian tubes or other problems. Special dye is injected into the uterus, and an X-ray is taken.
- Ovarian reserve testing. This helps your care team find out how many eggs you have for ovulation. The method often begins with hormone testing early in the menstrual cycle.
- Other hormone tests. These check the levels of hormones that control ovulation. They also check pituitary hormones that control processes involved in having a baby.
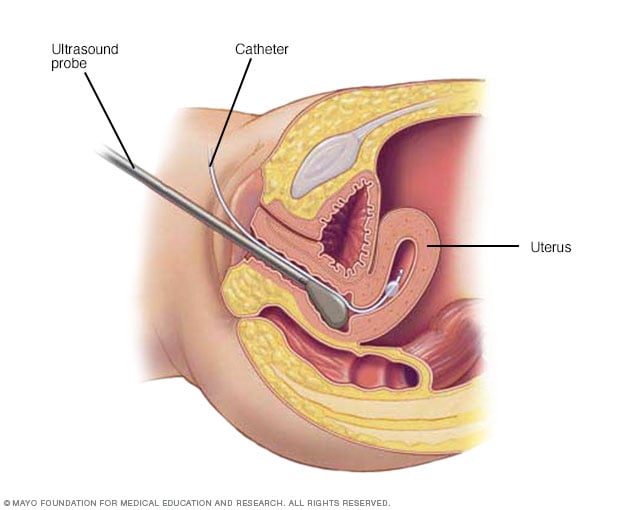
- Imaging tests. Pelvic ultrasound looks for diseases of the uterus or ovaries. Sometimes a test called a saline infusion sonogram is used to see details inside the uterus that can't be seen on a regular ultrasound. Another name for the saline infusion test is a sonohysterogram (son-o-his-ter-OH-gram).
Rarely, testing may include:
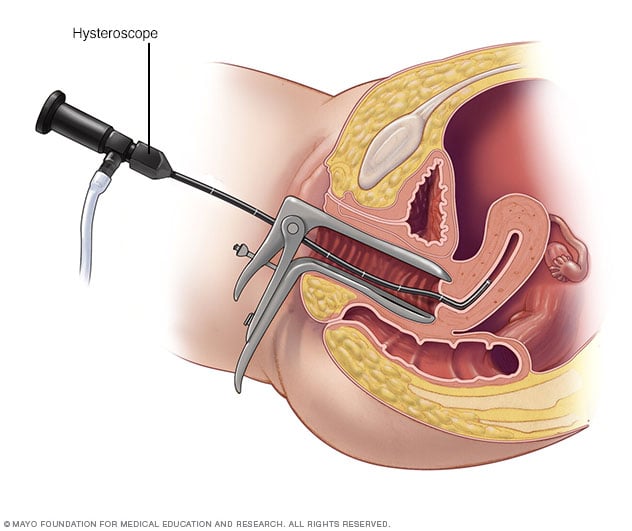
- Hysteroscopy. Depending on your symptoms, your health care team may use a hysteroscopy (his-ter-os-ko-pee) to look for a disease of the uterus. During the procedure, a thin, lighted device is placed through the cervix into the uterus to check for any irregular signs. It also can help guide minor surgery.
- Laparoscopy. Laparoscopy (lap-u-ros-kuh-pee) involves a small cut beneath the navel. Then a thin viewing device is placed through the cut to check the fallopian tubes, ovaries and uterus. The procedure may find endometriosis, scarring, blockages or other issues with the fallopian tubes. It also might find treatable problems with the ovaries and uterus. Laparoscopy is a type of surgery that can treat certain conditions as well. For example, it can be used to remove growths called fibroids or endometriosis tissue.
Not everyone needs to have all, or even many, of these tests before the cause of infertility is found. You and your health care team decide which tests you will have and when.
Treatment
Infertility treatment depends on:
- The cause of the infertility.
- How long you've been infertile.
- Your age and your partner's age, if you have a partner.
- Personal preferences.
Some causes of infertility can't be corrected.
If pregnancy doesn't happen after a year of unprotected sex, couples often can still become pregnant through infertility treatments called assisted reproductive technology. But treatment can involve big financial, physical, emotional and time commitments.
Treatment for men
Men's treatment for general sexual problems or a lack of healthy sperm may include:
- Lifestyle changes. Your health care team may recommend that you take the following steps. Have sex more often and closer to the time of ovulation. Get regular exercise. Drink less alcohol or give up harmful substances such as tobacco. Stop taking medicines that can affect fertility, but only if your health care team tells you to.
- Medicines. Your team may prescribe medicines to improve sperm count and boost the chances of a successful pregnancy. These prescription drugs may help the testicles function better too.
- Surgery. Sometimes, surgery may be able to reverse a sperm blockage and restore fertility. In other cases, repairing a large varicocele may improve the overall chances for pregnancy.
- Sperm retrieval procedures. These techniques can collect sperm if you can't ejaculate, or if no sperm is in your semen. Sperm retrieval procedures also may be used when assisted reproductive techniques are planned and sperm counts are low or irregular.
Treatment for women
Some women need only one or two treatments to improve fertility. Others may need a few types of therapies to become pregnant.
- Fertility medicines. These are the main treatments for infertility that's due to ovulation trouble. They can help the ovaries release an egg if ovulation is irregular or stops happening. Talk with your health care team about your options. Ask about the benefits and risks of each type of fertility medicine.
- Intrauterine insemination (IUI). With IUI, healthy sperm are placed directly in the uterus around the time that the ovary releases one or more eggs to be fertilized. Depending on the reasons for infertility, IUI can be timed with your menstrual cycle or with the use of fertility medicines. Your partner or a donor provides the sperm.
- Surgery to restore fertility. Some conditions of the uterus can be treated with hysteroscopy. These include polyps, scar tissue and some fibroids. Laparoscopic surgery with small cuts or traditional surgery with a large cut in the stomach area may be needed to treat conditions such as endometriosis, pelvic adhesions and larger fibroids.
Assisted reproductive technology
Assisted reproductive technology (ART) is any fertility treatment in which the egg and sperm are handled.
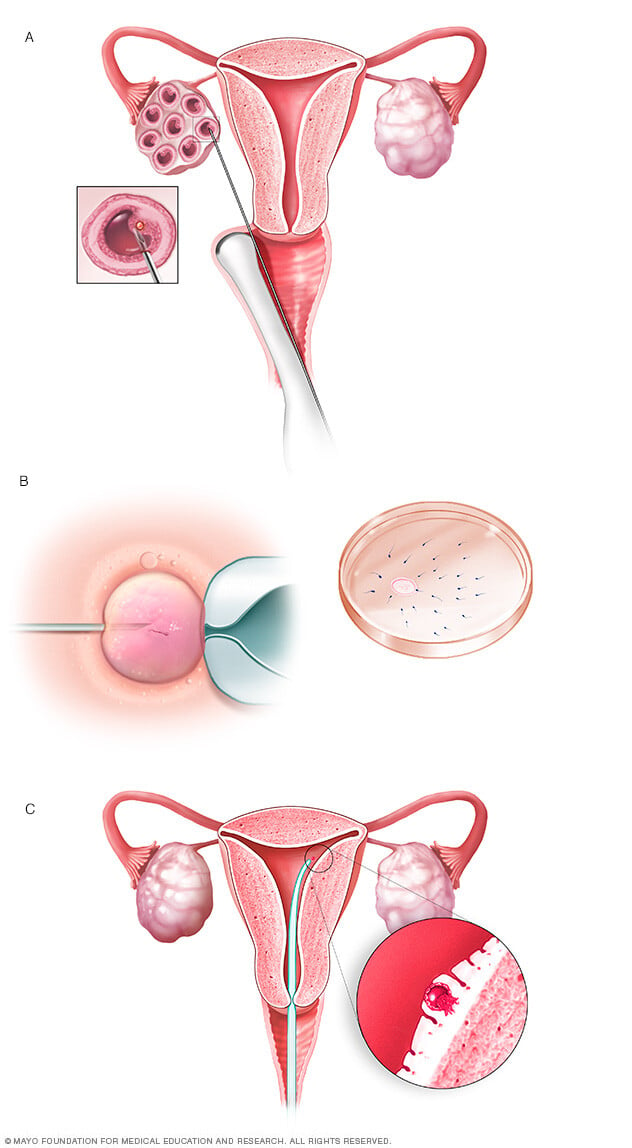
In vitro fertilization (IVF) is the most common ART technique. Some of the key steps in a cycle of IVF include:
- Fertility medicines are used to help the ovaries make eggs.
- Mature eggs are removed from the ovaries.
- The eggs are fertilized with sperm in a dish in a lab.
- The fertilized eggs, also called embryos, are placed in the uterus. Embryos also can be frozen for future use.
Sometimes, other techniques are used in an IVF cycle, such as:
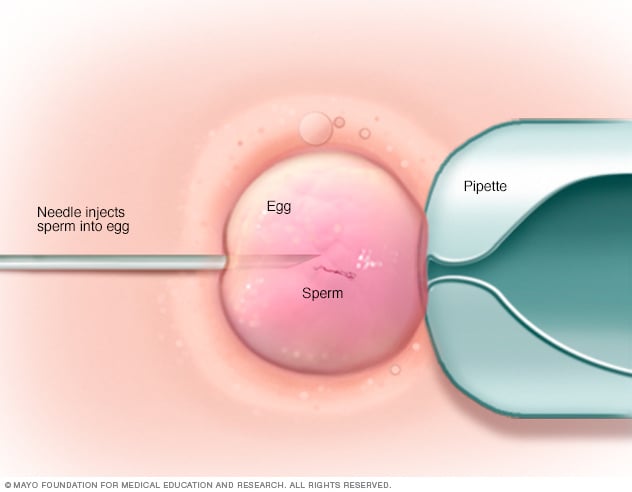
- Intracytoplasmic sperm injection (ICSI). A single healthy sperm is injected directly into a mature egg. Often, ICSI is used when semen quality or quantity is poor. Or it might be used if fertilization attempts during prior IVF cycles didn't work.
- Assisted hatching. This technique helps an embryo attach to the lining of the uterus. It opens part of the outer covering of the embryo, which is why it's called hatching.
- Donor eggs or sperm. Often ART is done using a couple's own eggs and sperm. But you have the choice to use eggs or sperm from a donor. This is an option if you're single or in a same-sex relationship. It's also done for medical reasons. These include poor egg quality due to age and sperm problems such as a blockage in the reproductive tract. Donor eggs or sperm also might be used if one partner has a genetic disease that could be passed on to a baby. An infertile couple can use donated embryos too. These come from other couples who received infertility treatment and had leftover embryos that were frozen.
- Gestational carrier. People who don't have a working uterus or for whom pregnancy poses a serious health risk might choose IVF using a gestational carrier. In this case, the couple's embryo is placed in the uterus of a person who agrees to carry the pregnancy.
- Genetic testing. Embryos made with IVF can be tested for genetic problems. This is called preimplantation genetic testing. Embryos that don't seem to have a gene problem can be placed in the uterus. This lowers the risk of a parent passing on a genetic condition to a child.
Complications of treatment
Complications of infertility treatment may include:
- Multiple pregnancy. The most common complication of infertility treatment is a multiple pregnancy — twins, triplets or more. A higher number of unborn babies in the womb raises the risk of premature labor and delivery. It also makes problems during pregnancy more likely, such as gestational diabetes. Babies born too early face worse odds of health and development challenges. Ask your health care team about all the risks of a multiple pregnancy before you start treatment.
- Ovarian hyperstimulation syndrome (OHSS). Fertility medicines can cause this condition in which the ovaries become swollen and painful. The risk of OHSS goes up with the use of assisted reproductive technologies such as in vitro fertilization. Symptoms can include mild pain in the stomach area, bloating and upset stomach that lasts about a week. Nausea may last longer if you become pregnant. Rarely, a more serious form of OHSS causes rapid weight gain and shortness of breath. This is an emergency that needs to be treated in the hospital.
- Bleeding or infection. Assisted reproductive technology or reproductive surgery comes with a risk of bleeding or infection.
Coping and support
Coping with infertility can be very hard, because there are so many unknowns. The journey can take a serious emotional toll. These steps can help you cope:
- Be prepared. The uncertainty of infertility testing and treatments can be stressful. Ask your fertility doctor to explain the steps and prepare for each one.
- Set limits. Before you start treatment, decide which procedures and how many you can afford financially and accept emotionally. Infertility treatments may be expensive and often are not covered by insurance companies. What's more, a successful pregnancy usually depends on more than one attempt at treatment.
- Think about other options. You might need to use donor sperm or eggs, or a gestational carrier. You could also consider adopting a child or choosing to have no children. Think about these options as early as possible in the infertility evaluation. It may ease anxiety during treatment and feelings of hopelessness if you don't become pregnant.
- Seek support. You might want to join an infertility support group or talk with a counselor before, during or after treatment. It can help you carry on through the process and ease grief if your treatment doesn't work.
Managing stress during treatment
Try these tips to help take charge of stress during infertility treatment:
- Express yourself. Reach out to others. It can help you deal with emotions such as anger, sadness or guilt.
- Stay in touch with loved ones. Talk to your partner, family or friends. The best support often comes from loved ones and those closest to you.
- Find ways to ease stress. Some studies suggest that people who get help managing stress during infertility treatment with ART have slightly better results than those who don't get help. Take steps to lower the stress in your life before you try to become pregnant. For instance, you could learn mindfulness meditation, practice yoga, keep a journal or make time for other hobbies that relax you.
- Exercise, eat a balanced diet and get enough sleep. These and other healthy habits can improve your outlook and keep you focused on living your life.
Managing emotional effects of the outcome
You may have emotional challenges no matter your results:
- Not getting pregnant or having a miscarriage. The stress of not being able to have a baby can be awful even in the most loving, supportive relationships.
- Success. Even if fertility treatment is successful, it's common to have stress and fear of failure during pregnancy. If you've had depression or anxiety in the past, you're at higher risk of those mental health conditions coming back in the months after your child's birth.
- Multiple births. A successful pregnancy that results in multiple births can add stress during pregnancy and after delivery.
Get professional help from a therapist if the emotional impact of infertility treatment, pregnancy or parenthood becomes too heavy for you or your partner.
Preparing for an appointment
Depending on your age and health history, your usual health care professional may recommend a medical evaluation. A gynecologist, urologist or family doctor can help find out whether there's a problem that requires a specialist or clinic that treats infertility problems. In some cases, both you and your partner may need a full infertility evaluation.
What you can do
To get ready for your first appointment:
- Note details about your attempts to get pregnant. Write down details about when you started trying to conceive and how often you've had sex, especially around the midpoint of your menstrual cycle — the time of ovulation.
- Bring your key medical information. Include any other health conditions that you or your partner has, as well as information about any previous infertility evaluations or treatments.
- Make a list of any medicines, vitamins, herbs or other supplements you take. Include the amounts you take, called the doses, and how often you take them.
- Make a list of questions to ask your health care team. List the most important questions first in case time runs short.
For infertility, some basic questions to ask your care team include:
- What kinds of tests do we need to find out why we haven't conceived yet?
- What treatment do you recommend we try first?
- What side effects might that treatment cause?
- What are the chances of having multiple babies with the treatment?
- How many times might we need to try this treatment before we conceive?
- If the first treatment doesn't work, what will you recommend trying next?
- Are there any long-term complications linked with this or other infertility treatments?
Feel free to ask your health care professional to repeat information or to ask follow-up questions.
What to expect from your doctor
Be ready to answer questions that your health care professional asks. Your answers can help your doctor figure out what tests and treatments you may need.
Questions for couples
Some questions that you and your partner may be asked are:
- How long have you been trying to get pregnant?
- How often do you have sex?
- Do you use any lubricants during sex?
- Do either of you smoke?
- Do either of you use alcohol or recreational drugs? How often?
- Are either of you taking any medicines, dietary supplements or anabolic steroids?
- Have either of you been treated for any other medical conditions, including sexually transmitted infections?
Questions for men
Your health care professional may ask:
- Do you have any trouble putting on muscle, or do you take any substances to increase muscle mass?
- Do you ever notice a fullness in the scrotum, especially after you stand for a long time?
- Do you have any testicle pain or pain after ejaculation?
- Have you had any sexual challenges, such as trouble keeping an erection, ejaculating too soon, not being able to ejaculate or having less sexual desire?
- Have you conceived a child with any previous partners?
- Do you often take hot baths or steam baths?
Questions for the woman
Your health care professional may ask:
- At what age did you get your menstrual period?
- What are your cycles typically like? How regular, long and heavy are they?
- Have you ever been pregnant before?
- Have you been charting your cycles or testing for ovulation? If so, for how many cycles?
- What is your typical daily diet?
- Do you exercise? How often?

