
Surgery for stress urinary incontinence in women
Stress urinary incontinence is the loss of bladder control when you exert pressure on your bladder by coughing, sneezing, laughing, exercising or lifting something heavy.
Usually, stress incontinence can be treated with a number of conservative treatments. These include lifestyle changes, exercises, weight loss or devices inserted into the vagina to support the bladder. When these options don't work, surgery may be an option for women with bothersome stress incontinence.
Although surgery has a higher risk of complications than other therapies, it may provide a long-term solution. Finding the best option for stress incontinence surgery depends on the benefits and risks associated with each procedure, as well as your particular health and treatment needs.
Treatment goal
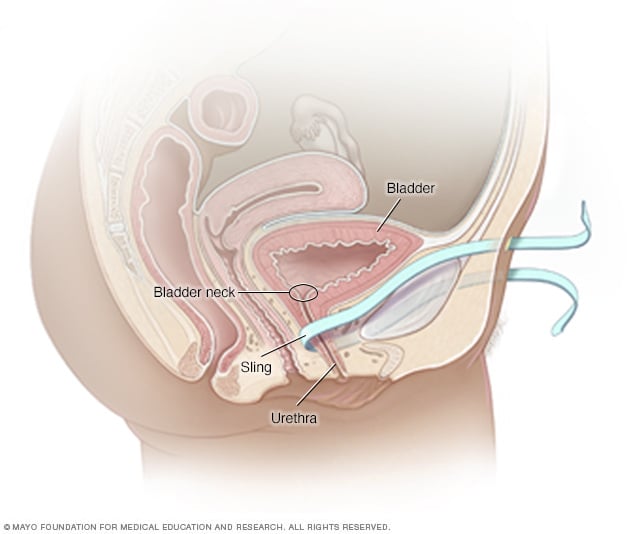
If you have stress incontinence, pressure on your bladder affects how well the urethra and bladder neck function. The urethra is the tube that carries urine out of the bladder. The bladder neck is where the urethra joins the bladder. A group of muscles called the external urethral sphincter help control the release of urine by closing the urethra.
The treatment goal of surgery is to support the urethra and bladder neck. This extra support helps keep the urethra closed when you exert pressure, so that you don't leak urine.
Possible risks
Like any surgery, urinary incontinence surgery comes with risks. Although uncommon, potential complications include:
- Temporary difficulty urinating
- Temporary difficulty emptying your bladder (urinary retention)
- Development of overactive bladder
- Urinary tract infection
- Wound infection
- Difficult or painful sex
- Surgical material sticking out into the vagina
- Groin pain
Talk to your health care professional and surgeon about the possible risks and benefits of your surgical options.
Other things to consider
Before deciding about surgery, consider these factors:
- Get an accurate diagnosis. Different types of incontinence require different therapies. Your health care provider might refer you to an incontinence specialist (urogynecologist or urologist) for further diagnostic testing.
- Understand that surgery only corrects the problem it's designed to treat. Surgery to treat stress incontinence doesn't treat the sudden, severe urge to urinate (overactive bladder). If you have mixed incontinence — a combination of stress incontinence and overactive bladder — you'll likely need additional treatments.
- Think about your plans for having children. Your doctor might recommend waiting for surgery until you're finished with childbearing. The strain of pregnancy and delivery on your bladder, urethra and supportive tissues might undo the benefits of a surgical fix.
Slings
The most common procedure uses a sling to support the urethra or bladder neck. The sling is usually made from a synthetic material or a strip of your own body tissue.
Your surgeon will discuss the benefits and risks of different surgical materials and different approaches for the placement of a sling. Although rare, a synthetic mesh may erode.
Recovery times will vary with different procedures. Your surgeon may recommend 2 to 6 weeks of healing before you return to regular daily activities. You'll also receive instructions on when you can resume exercise and sexual activity.
Tension-free slings
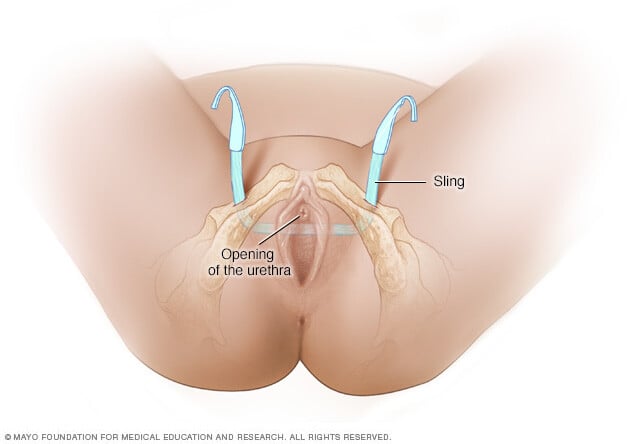
A tension-free sling is a mesh usually made from a synthetic material called polypropylene. To support the urethra, the sling functions like a hammock and is held in place by body tissues rather than stitches. During the healing process, scar tissue forms in and around the mesh to keep it from moving.
For a tension-free sling procedure, your surgeon will likely recommend one of these approaches:
- Retropubic procedure. The surgeon makes a small cut (incision) inside the vagina to have access to the urethra. There are also two small incisions above the pubic bone, just to the right and left of the center. The surgeon uses a needle to pass each end of the sling from the vagina to abdomen. The sling is held in place by the soft tissue along its path. Absorbable stitches close the vaginal incision, and the incisions on the skin may be sealed with glue or stitches.
- Transobturator procedure. The surgeon makes a small incision in the vagina and small incisions in the right and left groin. The surgical process is similar to the retropubic approach, but the mesh passes through the groin muscles rather than the abdominal wall.
Both sling procedures are safe and effective. But the transobturator sling may not work as well if you also need other procedures to fix pelvic floor problems.
Another tension-free sling is the single-incision mini procedure. The surgeon makes a single small cut in the vagina. A small mesh hammock is suspended from tissues the pelvic region. The surgeon takes care to avoid the groin muscles. The results of the single-incision mini procedure are generally less effective. More research is needed to determine the safety and effectiveness of this method.
Conventional slings
A conventional sling uses tissue from your own body to support the bladder neck. The surgeon collects the tissue to make the sling from either your abdomen or thigh. The surgeon then makes an incision in the vagina to place the sling below the urethra at the bladder neck. From an incision in the abdomen, the surgeon stitches each end of the sling to the abdominal wall.
A conventional sling typically requires a larger incision than a tension-free sling. You might need an overnight stay in a hospital and usually a longer recovery period. You may also need a temporary catheter after surgery while you heal.
This procedure is associated with a higher risk of difficulty emptying the bladder. Therefore, it's typically reserved for women who have had another incontinence procedure but still experience urinary incontinence.
Suspension procedures
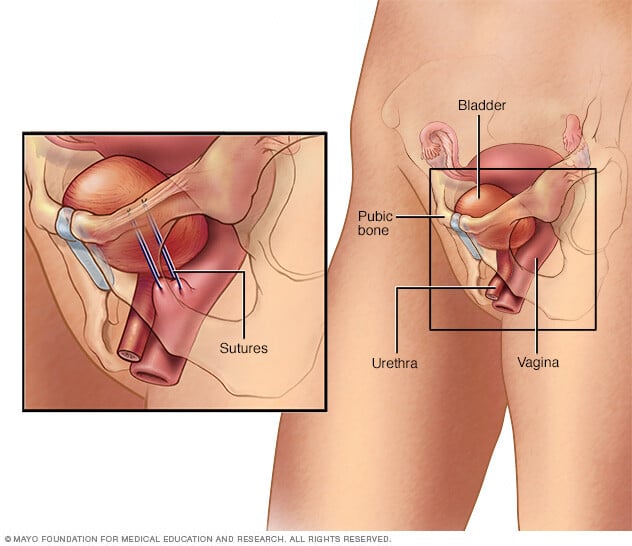
Suspension procedures provide support for the urethra or bladder neck by lifting tissues around the urethra toward structures in the pelvis.
The most common method is the Burch procedure. The surgeon attaches one end of surgical threads to the outer wall of the vagina and the other end to ligaments near the top of the pelvic bone. The stitches (sutures) essentially suspend the vagina to the pelvic ligament. When the sutures are tightened, the vagina is shifted up to support the bladder neck from below.
Suspension procedures are performed through an incision in the lower abdomen or through several small incisions (laparoscopic surgery). With a laparoscopic procedure, the surgeon uses a video camera and tiny instruments attached to tubes. This usually results in a shorter recovery period, but laparoscopic surgery may not be as effective as an open procedure.
One step at a time
Finding an effective remedy for stress urinary incontinence might take time, with several steps along the way. If a conservative treatment isn't working for you, ask your doctor if there might be a surgical option for you.

